SITE OF LESION-upper brain stem
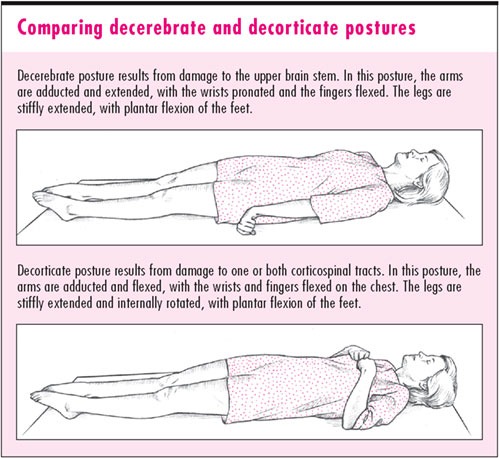
POSTURE-the arms are adducted and extended, with the wrists pronated and the fingers flexed. The legs are stiffly extended, with plantar flexion of the feet.
In severe cases, the back is acutely arched (opisthotonos).
CAUSED BY-
1)VASCULAR-infarction(Brain stem), hemorrhage(Pontine,Posterior fossa)
2)MECHANICAL-tumor,abscess,any cerebral lesion that increases ICP may also produce decerebrate posture
3)METABOLIC-encephalopathy(Hepatic,Hypoglycemic,Hypoxic)
4)ACCIDENTAL-Removal of spinal fluid during a lumbar puncture to relieve high ICP may lead to cerebral compression of the brain stem
4)TRAUMA-Head trauma
URGENT-maintain airway or insert artificial airway and provide positive pressure repiration with measures to prevent aspiration as necessary.
POINTS TO NOTE-
A)Decerebrate posturing indicates the second-lowest measure of motor response, according to the GLASGOW COMA SCALE.
B)Decerbrate posture is relatively a late manifestation(i.e. preceded by other discernable signs and symptoms) in-
Brain stem tumor,Cerebral lesion,Hepatic encephalopathy,Hypoglycemic encephalopathy,etc.(i.e. in problems other than accidental and vascular)
C)Decerebrate posture sets early in Pontine hemorrhage,Posterior fossa hemorrhage,Brain stem infarction.(i.e. in vascular problems)
D)CHILDREN YOUNGER THAN 2YRS MAY NOT EXHIBT DECORTICATE POSTURE DUE TO IMMATURE CNS.BUT OFTEN IT PRESENT AS SEVERE OPISTHOTONOS AND IS USUALLY A TERMINAL SIGN AND THE MOST COMMON CAUSE BEING HEAD TRAUMA.IT CAN ALSO OCCUR IN REYE’S SYNDROME AS A RESULT OF INCREASED ICP CAUSING BRAIN STEM COMPRESSION.
HISTORY AND PHYSICAL EXAMINATION-
must include-
Vital signs,
Level of consciousness (LOC) preferably using GCS,
Pupil- size,equality, and response to light.
Deep tendon reflexes (DTRs) and
Cranial nerve reflexes, and
check for Doll's eye sign.
Next, explore the history of the patient's coma. If you're unable to obtain this information, look for clues to the causative disorder, such as hepatomegaly, cyanosis, diabetic skin changes, needle tracks, or obvious trauma. If a family member is available, find out when the patient's LOC began deteriorating. Did it occur abruptly? What did the patient complain of before he lost consciousness? Does he have a history of diabetes, liver disease, cancer, blood clots, or aneurysm? Ask about any accident or traumatic injury responsible for the coma.
INVESTIGATIONS-
Radiological-skull x-ray,CT scan,MRI,Cerebral angiography,Digital substraction angiography.
Other-EEG,Brain scan,ICP monitoring
MONITOR-neurologic status and vital signs every 30 minutes or as indicated.
Also be alert for signs of increased ICP (bradycardia, increasing systolic blood pressure, and widening pulse pressure) and neurologic deterioration (altered respiratory pattern and abnormal temperature).